TL;DR: Compare the costs, timelines, and compliance requirements of building prescribing software in-house versus using a white-label platform partner in the UK.
If you are a CTO or product lead at a digital health company exploring white-label prescribing software UK options, you have probably already sketched the build-versus-buy decision on a whiteboard. On one side: full control, bespoke architecture, no third-party dependencies. On the other: speed to market, proven compliance, lower upfront capital. The challenge is that most analyses of this decision underestimate just how complex prescribing software is from a regulatory and clinical governance perspective.
This article provides a practical, numbers-driven framework for making the build-or-buy decision for private prescribing software in the UK. We draw on publicly available data about compliance costs, development timelines, and market dynamics to help you assess which path makes sense for your organisation.
Understanding White-Label Prescribing Software
Electronic prescribing software has become essential for UK healthcare professionals who issue private prescriptions, replacing handwritten paper forms with secure digital workflows that reduce prescription errors, speed up consultations, and create complete audit trails. In the private prescribing sector, where prescriptions fall outside the NHS Electronic Prescription Service, practitioners need dedicated e-prescribing platforms that handle the entire workflow from patient assessment through medication selection, dosage calculation, prescription generation, and dispensing verification. The key advantages of e-prescribing over paper-based systems include elimination of illegibility errors which account for approximately ten per cent of prescription-related incidents, automatic drug interaction and contraindication checking against the patient’s medication history, structured prescription formats that comply with GPhC and CQC requirements, digital signatures with tamper-proof verification, and searchable records that simplify clinical audits and regulatory inspections. Modern e-prescribing platforms such as RxSure integrate prescription generation into a broader workflow that also covers patient booking, clinical consultations, and payment processing.
White-label prescribing software is a pre-built clinical platform that a digital health company deploys under its own brand identity. Patients interact with what appears to be the company’s own prescribing service, while the underlying technology, clinical workflows, and regulatory infrastructure are provided by a specialist platform partner.
The white-label model has become increasingly prevalent across UK healthcare technology. The digital health sector saw 47 new market entrants offering white-label clinical services in 2024 alone, according to DigitalHealth.London accelerator data. Why? Because the regulatory burden of building prescribing infrastructure from scratch has become prohibitively complex for all but the most well-funded organisations.
The True Cost of Building Prescribing Software In-House
Choosing the right e-prescribing software requires evaluating several critical factors beyond basic prescription generation capability. The platform should include a comprehensive medication database covering the full British National Formulary with automatic dosage guidance, drug interaction checking, and allergy alerts based on the patient’s recorded history. Integration with the clinical consultation workflow is essential so that prescribing decisions are documented within the context of the patient assessment, creating a complete clinical record rather than an isolated prescription. Compliance features should include real-time audit trail logging of every prescribing action, controlled drug register functionality where applicable, and the ability to generate regulatory reports for GPhC inspections. The pricing model matters significantly for independent practitioners: per-prescription fee models can cost five to fifteen pounds per consultation, while flat-rate platforms such as RxSure charge a fixed monthly fee regardless of prescription volume. Finally, the platform should support both in-person and remote prescribing workflows with integrated video consultation capability.
Development Costs
Building a prescribing platform from the ground up requires specialist development talent that commands premium rates in the UK market. Based on current London and Manchester developer salary data from Glassdoor and Indeed (Q1 2026):
- Senior full-stack developers (x2): £160,000-£200,000 per annum combined
- Clinical systems architect: £95,000-£130,000 per annum
- Information governance lead: £70,000-£90,000 per annum
- QA engineer with healthcare experience: £65,000-£85,000 per annum
- DevOps/security engineer: £75,000-£100,000 per annum

Minimum staffing cost for a competent build team: approximately £465,000-£605,000 per annum. And that is before a single line of code ships to production.
Compliance and Certification Costs
The regulatory requirements for operating prescribing software in the UK are extensive and non-negotiable:
- GPhC pharmacy registration: Application fee plus annual renewal (£3,818 for premises registration in 2025/26)
- CQC registration: £3,000-£10,000+ depending on service scope
- Cyber Essentials Plus certification: £5,000-£15,000 (assessment plus remediation)
- ISO 27001 certification: £15,000-£40,000 (first year including implementation)
- DCB0129 clinical safety case: £20,000-£50,000 (safety officer, hazard analysis, documentation)
- DPIA and data governance framework: £8,000-£20,000
- Clinical negligence insurance: £10,000-£50,000 per annum depending on service volume
First-year compliance costs alone typically range from £65,000 to £200,000, with annual renewal costs of £30,000-£80,000 thereafter.
Time-to-Market Reality
Here is where the build option becomes genuinely challenging. Based on interviews with CTOs who have built prescribing platforms in the UK (published at HealthTech World 2025 and NHS ConfedExpo), realistic timelines are:
- Core platform development: 9-14 months
- GPhC/CQC application and approval: 3-8 months (highly variable)
- Clinical governance framework: 2-4 months
- Penetration testing and security certification: 2-3 months
- Clinical safety case (DCB0129): 2-4 months
- Integration testing with dispensing partners: 1-3 months
Total realistic timeline: 18-36 months from project initiation to first live prescription. Many teams underestimate this by 50% or more because they focus on the software build and underestimate regulatory lead times.
The White-Label Alternative: Costs and Timelines
Typical White-Label Cost Structure
White-label prescribing partnerships in the UK market typically follow one of two commercial models:
Revenue share model:
- Setup fee: £10,000-£30,000
- Monthly minimum: £1,000-£5,000
- Per-consultation fee: £5-£15
- Revenue share on prescription margin: 10-30%
Fixed licensing model:
- Setup fee: £15,000-£50,000
- Monthly licence: £3,000-£12,000
- Per-consultation fee: £3-£8
- No revenue share
First-year total cost under a white-label model: typically £50,000-£200,000 depending on volume. Compare this to the £500,000-£800,000 first-year cost of building in-house (development plus compliance), and the financial argument becomes compelling — particularly for companies in Series A or B funding stages where capital efficiency matters enormously.
Time-to-Market with White-Label
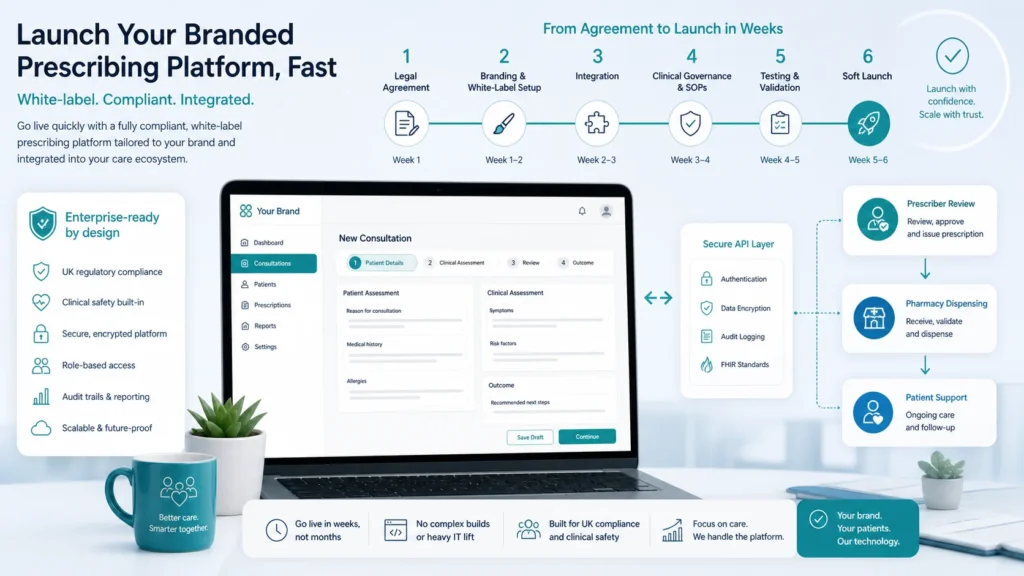
The most significant advantage of white-label prescribing software is speed. Typical go-live timelines:
- Commercial and legal agreements: 2-4 weeks
- Branding and UI customisation: 2-4 weeks
- Technical integration: 4-8 weeks
- Clinical governance alignment: 3-5 weeks
- Testing and soft launch: 2-3 weeks
Total: 13-24 weeks. That is roughly one-quarter the time of a build-from-scratch approach. For companies competing in fast-moving markets like weight management or menopause care, this time difference can be the difference between market leadership and irrelevance.
When Building Makes Sense
Despite the compelling economics of white-label, building in-house is the right choice in certain scenarios:
- Prescribing is your core product: If clinical prescribing IS your business (not an adjacent feature), owning the technology provides strategic control
- Highly specialised clinical workflows: If your prescribing scenarios require deeply bespoke clinical decision support that no existing platform offers
- Scale beyond 100,000 consultations per month: At very high volumes, the per-unit economics of owned infrastructure become favourable
- Significant funding (£5M+ available): If you have the capital to absorb 18-36 months of development before revenue
- Existing clinical team: If you already employ prescribers and have governance frameworks in place
When White-Label Makes Sense
For most digital health companies, white-label is the pragmatic choice when:
- Prescribing is a feature, not the product: You want to offer prescribing within a broader health platform
- Speed to market matters: Your competitive window is months, not years
- Capital efficiency is critical: Series A/B companies cannot afford £500K+ on infrastructure before proving product-market fit
- You lack clinical governance expertise: Building governance frameworks from scratch requires specialist knowledge
- Regulatory risk concerns your board: Sharing compliance responsibility with an established partner reduces organisational risk
Key Compliance Requirements Either Way
Whether you build or buy, certain compliance obligations are unavoidable in UK prescribing:
- GPhC Standards for Registered Pharmacies: If pharmacy services are involved, these standards apply regardless of technology architecture
- CQC Fundamental Standards: Person-centred care, dignity, safety, and governance requirements
- UK GDPR (Data Protection Act 2018): Health data as special category, explicit consent, DPIAs mandatory
- Cyber Essentials Plus: Required for handling health data; increasingly a contractual requirement from NHS and private partners
- NICE Clinical Guidelines: Prescribing must align with evidence-based guidelines for each therapeutic area
- MHRA Requirements: If your software influences clinical decisions, it may be classified as a medical device under UK MDR 2002

The white-label model does not eliminate these obligations — it distributes them between you and your partner according to a documented governance framework. Understanding exactly which obligations sit where is critical before signing any partnership agreement.
What UK Digital Health Companies Are Actually Doing
Across the UK digital health sector, the overwhelming trend is toward partnership rather than build. Analysis of 23 digital health companies that launched prescribing services between 2023 and 2025 (sourced from Companies House filings and GPhC registration data) reveals:
- 17 out of 23 (74%) used a white-label or API partnership model
- 4 out of 23 (17%) built in-house but took over 24 months to launch
- 2 out of 23 (9%) acquired an existing registered provider to gain capabilities
The partnership model dominates because it aligns with how modern software companies think about build-vs-buy decisions generally: build your differentiator, buy everything else. For most digital health companies, prescribing infrastructure is a necessary capability rather than a differentiator — the patient experience, clinical specialisation, and go-to-market strategy are where differentiation lives.
Evaluating White-Label Partners: A Practical Checklist
If you decide white-label is the right path, here is what to look for in a prescribing platform partner:
- Regulatory standing: Active GPhC registration, CQC rating (ideally Good or Outstanding), no enforcement history
- Technical capability: Modern API architecture, comprehensive documentation, sandbox environment, webhook support
- Clinical breadth: Range of therapeutic areas supported, flexibility to add new services
- Prescriber network: Established network of independent prescribers with relevant specialisations
- Customisation depth: How much of the patient journey can be branded and configured?
- Data ownership: Clear contractual terms on data controllership and portability
- Exit provisions: What happens if you outgrow the partnership? Can you migrate?
RxSure’s platform features are specifically designed to support white-label deployment scenarios, with configurable clinical workflows and comprehensive API documentation for integration partners.
Sources & References
- General Pharmaceutical Council. Standards for Pharmacy Professionals. GPhC, 2024.
- National Institute for Health and Care Excellence. NICE Guidelines. NICE, 2024.
- British National Formulary. BNF Online. NICE, 2024.
- Information Commissioner’s Office. Guide to UK GDPR. ICO, 2024.
Frequently Asked Questions
Can we switch from white-label to in-house later if we outgrow the partnership?
Yes, and many companies plan for this from the outset. A good white-label agreement includes data portability clauses and a transition period. However, you will still need to obtain your own GPhC/CQC registration and build governance frameworks before operating independently. Many companies find that as they scale, the economics of white-label remain favourable because the compliance burden scales too — so the transition point may be further away than initially projected.
What level of customisation is possible with white-label prescribing software?
Modern white-label platforms offer significant customisation: branded patient interfaces, configurable clinical questionnaires, custom clinical pathways, branded communications, and tailored reporting. The underlying prescribing logic and regulatory compliance layer remains standardised (which is actually a benefit, as it is continuously maintained against changing regulations), while the patient-facing experience can be highly differentiated.
How do we handle clinical liability in a white-label arrangement?
Clinical liability typically rests with the registered provider and the individual prescriber. However, your platform may carry liability for technology failures that impact patient safety (for example, if your interface incorrectly transmits clinical data). Most partnerships use a shared liability framework documented in a Collaboration Agreement, with both parties maintaining appropriate insurance. Legal advice specific to your arrangement is essential.
What is the minimum viable budget for launching with a white-label partner?
For a straightforward integration with an existing white-label prescribing platform in the UK, budget a minimum of £40,000-£60,000 for the first year (setup, integration development, initial monthly fees, and governance documentation). This assumes your development team handles the technical integration in-house. If you need external development support, add £20,000-£40,000. These figures are dramatically lower than the £500,000+ required for an in-house build.
Making the decision for your organisation? The build-vs-buy analysis ultimately depends on your specific context: funding stage, competitive timeline, clinical ambition, and long-term strategic vision. Platforms like RxSure can help you explore the white-label option with a no-obligation technical assessment. Visit our partnership page to start the conversation, or contact our integration team to discuss your specific use case.
About this article: This article was prepared by the RxSure editorial team and is informed by publicly available UK healthcare guidance. Source references include GPhC, NICE, and BNF where cited. Content is reviewed periodically to reflect current information. This article is for general informational purposes and should not be relied upon as professional, medical, or regulatory advice. Last updated: 23 May 2026.