
TL;DR: Technical guide to integrating e-prescribing into UK telehealth platforms. Covers API architecture, clinical governance, GDPR, and NHS DSPT requirements.
The UK Telehealth Boom and the Prescribing Gap
Electronic prescribing software has become essential for UK healthcare professionals who issue private prescriptions, replacing handwritten paper forms with secure digital workflows that reduce prescription errors, speed up consultations, and create complete audit trails. In the private prescribing sector, where prescriptions fall outside the NHS Electronic Prescription Service, practitioners need dedicated e-prescribing platforms that handle the entire workflow from patient assessment through medication selection, dosage calculation, prescription generation, and dispensing verification. The key advantages of e-prescribing over paper-based systems include elimination of illegibility errors which account for approximately ten per cent of prescription-related incidents, automatic drug interaction and contraindication checking against the patient’s medication history, structured prescription formats that comply with GPhC and CQC requirements, digital signatures with tamper-proof verification, and searchable records that simplify clinical audits and regulatory inspections. Modern e-prescribing platforms such as RxSure integrate prescription generation into a broader workflow that also covers patient booking, clinical consultations, and payment processing.
Telehealth prescribing integration has become a strategic priority for digital health platforms operating in the UK market. The COVID-19 pandemic accelerated telehealth adoption by a decade — NHS Digital reported that 58% of GP consultations were delivered remotely at peak lockdown in 2020, and while that figure has normalised to approximately 30% in 2024, the expectation of digital-first healthcare is now embedded in patient behaviour.
Yet many telehealth platforms face a critical gap in their clinical workflow: they can assess, diagnose, and advise patients remotely, but cannot close the loop with a prescription. Patients are directed back to their GP for a prescription, creating friction that undermines the very convenience telehealth promises. For platforms serving private patients, this gap represents both a clinical limitation and a commercial constraint.
The opportunity is substantial. The UK private telehealth market was valued at £850 million in 2023 and is projected to reach £2.1 billion by 2028, according to Precedence Research. Platforms that integrate prescribing capability capture significantly more value per consultation while delivering a genuinely complete patient experience.
Understanding the UK E-Prescribing Landscape
Choosing the right e-prescribing software requires evaluating several critical factors beyond basic prescription generation capability. The platform should include a comprehensive medication database covering the full British National Formulary with automatic dosage guidance, drug interaction checking, and allergy alerts based on the patient’s recorded history. Integration with the clinical consultation workflow is essential so that prescribing decisions are documented within the context of the patient assessment, creating a complete clinical record rather than an isolated prescription. Compliance features should include real-time audit trail logging of every prescribing action, controlled drug register functionality where applicable, and the ability to generate regulatory reports for GPhC inspections. The pricing model matters significantly for independent practitioners: per-prescription fee models can cost five to fifteen pounds per consultation, while flat-rate platforms such as RxSure charge a fixed monthly fee regardless of prescription volume. Finally, the platform should support both in-person and remote prescribing workflows with integrated video consultation capability.
Before diving into integration considerations, it is essential to understand the regulatory and technical landscape of prescribing in the UK.
The Electronic Prescription Service (EPS)
NHS England’s Electronic Prescription Service handles over 1.4 billion prescription items annually. EPS allows prescribers to send prescriptions electronically to a patient’s nominated pharmacy, eliminating paper tokens. However, EPS is designed for NHS prescribing and requires specific accreditation, Spine connectivity, and integration with the NHS Personal Demographics Service (PDS).
Private prescriptions operate outside EPS. While the NHS Long Term Plan envisions eventual integration of private prescribing into electronic systems, the current reality is that private prescriptions are typically generated as PDF documents, issued via secure digital delivery, or in some cases still printed. This creates an integration opportunity for platforms willing to build robust private prescribing workflows.
Who Can Prescribe?
In the UK, prescribing authority extends beyond doctors to include:
- Pharmacist independent prescribers — registered with the GPhC, able to prescribe any medicine within their competence
- Nurse independent prescribers — registered with the NMC, similar scope to pharmacist IPs
- Supplementary prescribers — prescribe within an agreed clinical management plan
- Dentists — within dental conditions
- Optometrists — for ocular conditions (independent prescriber qualified)
This breadth of prescribing professionals creates opportunities for telehealth platforms to access prescribing capability without necessarily employing doctors — a significant consideration for both cost management and scalability.
API Integration Considerations for Telehealth Prescribing
Integrating prescribing into an existing telehealth platform requires careful architectural decisions. The core question is: build or integrate? Building a prescribing engine from scratch means handling clinical decision support, drug interaction checking, formulary management, prescription generation, and regulatory compliance internally. Integrating with a specialist prescribing platform means leveraging existing, tested infrastructure via API.
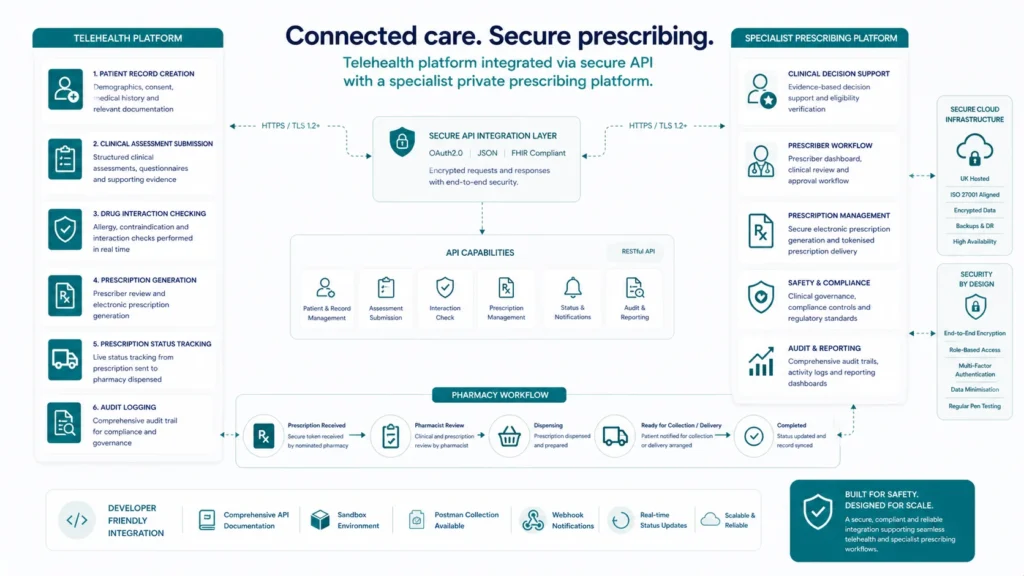
Key API Capabilities Required
- Patient record creation and retrieval — creating prescribing records linked to your platform’s patient identifiers, with demographic verification
- Clinical assessment submission — passing structured consultation data (symptoms, history, examination findings) to the prescribing system
- Drug interaction and contraindication checking — real-time clinical decision support against the patient’s medication history
- Prescription generation — creating legally valid private prescriptions with all required elements (prescriber details, GMC/GPhC number, date, directions)
- Prescription status tracking — monitoring whether a prescription has been viewed, dispensed, or is pending collection
- Audit logging — comprehensive, immutable records of all prescribing activity for regulatory compliance
Platforms like RxSure offer API-first architectures designed specifically for this type of integration, reducing time-to-market from years to months.
Clinical Governance Requirements for Remote Prescribing
The CQC, GPhC, and GMC all publish guidance on remote prescribing that any integrated platform must satisfy. These are not suggestions — they are regulatory requirements with serious consequences for non-compliance.
Key governance requirements include:
- Patient identity verification — robust processes to confirm the patient is who they claim to be. The GPhC specifically highlights this for remote consultations where visual verification is limited.
- Adequate clinical assessment — the CQC expects that remote consultations gather sufficient information to make safe prescribing decisions. This may require video capability, not just text-based chat.
- Access to patient records — prescribers should, where possible, access the patient’s Summary Care Record or equivalent to check medication history, allergies, and relevant conditions.
- Prescribing within competence — the platform must ensure prescribers only prescribe within their declared areas of competence, with technical controls to enforce this.
- Clinical supervision and peer review — independent prescribers operating remotely need access to clinical supervision, peer discussion, and escalation pathways.

Your platform architecture must embed these requirements into the clinical workflow, not rely on prescriber discipline alone. Mandatory fields, competence-based access controls, and automated escalation triggers are the minimum standard.
Data Security: GDPR, NHS DSPT, and Beyond
Healthcare data is among the most sensitive personal data processed in the UK. Any platform handling prescribing data must meet stringent security requirements — failure to do so risks ICO enforcement action, reputational damage, and criminal prosecution under the Computer Misuse Act.
GDPR Compliance for Health Data
Health data is classified as special category data under UK GDPR Article 9, requiring explicit consent or another lawful basis for processing. Prescribing data — including medication names, dosages, and clinical conditions — is unambiguously health data. Your platform must implement:
- Lawful basis documentation (typically explicit consent for private healthcare or legitimate interests with DPIA)
- Data minimisation — only collecting data necessary for prescribing decisions
- Storage limitation — clear retention policies aligned with professional record-keeping requirements (typically 10 years for adults)
- Right to access and portability — patients must be able to obtain their prescribing records
- Data Protection Impact Assessment — mandatory for large-scale health data processing
NHS Data Security and Protection Toolkit (DSPT)
If your platform integrates with any NHS systems (SCR access, PDS lookups, or referral pathways), DSPT compliance is mandatory. Even for purely private platforms, achieving DSPT standards demonstrates security maturity to partners, regulators, and patients. The toolkit covers ten data security standards across leadership, training, technology, and incident response.
Technical security measures should include end-to-end encryption for data in transit, AES-256 encryption at rest, multi-factor authentication for all prescriber access, role-based access controls, and penetration testing at least annually. Hosting should be within UK data centres with ISO 27001 certification.
User Journey Mapping: From Consultation to Dispensing
How does the integrated prescribing journey actually feel for your users? Mapping this end-to-end is critical for both user experience and clinical safety.
- Step 1: Patient booking — patient selects consultation type, completes pre-screening questionnaire, verifies identity
- Step 2: Clinical consultation — video or synchronous chat consultation with the prescriber, documented in real time within the platform
- Step 3: Prescribing decision — prescriber selects medication, dose, and quantity from the formulary. System performs interaction and contraindication checks automatically.
- Step 4: Prescription generation — platform generates a legally valid private prescription with all required elements, digitally signed by the prescriber
- Step 5: Prescription delivery — prescription sent electronically to patient’s chosen pharmacy, or dispensed directly if the platform includes pharmacy services
- Step 6: Dispensing confirmation — pharmacy confirms dispensing, closing the loop and updating the patient record
- Step 7: Follow-up — automated follow-up scheduling for ongoing treatment, triggered by platform logic

Each step must be instrumented with audit logging, error handling, and timeout management. What happens if the prescriber loses connectivity mid-consultation? What if the pharmacy cannot source the medication? Your platform must handle edge cases gracefully.
The Build vs. Integrate Decision
For most telehealth platforms, building prescribing capability from scratch is prohibitively expensive and slow. The regulatory knowledge alone — understanding private prescription legal requirements, controlled drug regulations, prescribing formulary management — represents years of specialist expertise. Add clinical decision support development, drug database licensing (dm+d integration), and ongoing regulatory maintenance, and the build cost easily exceeds seven figures.
Integration with an established prescribing platform offers a faster path to market with lower risk. The key evaluation criteria should include:
- API documentation quality and developer experience
- Clinical governance framework included or required separately
- Regulatory status — is the provider already registered with CQC or GPhC?
- Scalability — can the platform handle your growth projections?
- White-label capability — does the prescribing journey feel native to your brand?
- Commercial model — per-prescription fees, monthly licensing, or revenue share?
View RxSure’s partnership pricing for an example of how integration commercial models can work for telehealth platforms of different scales.
Frequently Asked Questions
Do we need our own CQC registration to integrate prescribing?
It depends on your model. If prescribers are employed by your platform and you direct their clinical activity, you likely need CQC registration as a provider of regulated activity. If you integrate with a separately registered prescribing service (where prescribers are governed by that service’s clinical framework), the CQC registration sits with the prescribing partner. Most telehealth platforms choose the integration model initially, as CQC registration adds 3-6 months to launch timelines and significant ongoing compliance overhead.
What drug database should we use for clinical decision support?
The NHS Dictionary of Medicines and Devices (dm+d) is the UK standard for medication identification. For clinical decision support (interactions, contraindications, dosing), commercial databases such as the BNF API, First Databank, or Medicines Complete provide structured, maintained data. Licensing costs vary but are essential — building your own interaction database is neither safe nor practical. An integrated prescribing platform will typically include drug database access within their service.
How long does a typical integration take?
For a well-documented API with good developer support, expect 8-12 weeks for a basic integration covering the core prescribing workflow. Add 4-6 weeks for clinical governance documentation, prescriber onboarding, and testing. End-to-end, most platforms achieve first live prescription within 4-6 months of project initiation. Complex integrations with custom clinical pathways, multiple prescriber types, or high-volume requirements may take longer.
Can we offer controlled drug prescribing through a telehealth integration?
Controlled drugs (Schedules 2-5) carry additional legal requirements under the Misuse of Drugs Regulations 2001. Schedule 2 and 3 drugs require specific prescription formats, cannot be transmitted electronically in most cases, and have quantity limitations. While not impossible to offer via telehealth, the regulatory complexity and abuse risk mean most platforms exclude CDs initially and add them later with enhanced clinical governance controls. The Home Office and CQC both scrutinise remote CD prescribing closely.
Sources & References
- General Pharmaceutical Council. Standards for Pharmacy Professionals. GPhC, 2024.
- National Institute for Health and Care Excellence. NICE Guidelines. NICE, 2024.
- British National Formulary. BNF Online. NICE, 2024.
- Information Commissioner’s Office. Guide to UK GDPR. ICO, 2024.
Getting Started with Prescribing Integration
Adding e-prescribing to your telehealth platform transforms your clinical offering from advice-only to complete care delivery. The technical integration is achievable within months, but success depends equally on clinical governance preparation, regulatory understanding, and choosing the right prescribing partner.
If your telehealth platform is ready to explore prescribing integration, start by reviewing the RxSure partnership programme for technical and commercial details, or contact our integration team directly to discuss your platform architecture and timeline. We work with telehealth platforms of all sizes, from early-stage startups to established NHS-adjacent providers.
About this article: This article was prepared by the RxSure editorial team and is informed by publicly available UK healthcare guidance. Source references include GPhC, NICE, and BNF where cited. Content is reviewed periodically to reflect current information. This article is for general informational purposes and should not be relied upon as professional, medical, or regulatory advice. Last updated: 23 May 2026.


