TL;DR: Platform requirements for pharmacy groups scaling GLP-1 weight management services across multiple sites. Cold chain, monitoring, and clinical governance.
The UK Obesity Crisis and the Rise of GLP-1 Prescribing
Weight management services represent one of the fastest-growing revenue opportunities for UK community pharmacies, driven by rising demand for GLP-1 receptor agonist medications such as semaglutide (Wegovy) and tirzepatide (Mounjaro) alongside established treatments including orlistat. Pharmacist independent prescribers are ideally positioned to deliver these services because they combine clinical expertise with patient accessibility, offering consultations during extended pharmacy opening hours without the waiting times associated with GP referrals. A structured weight management consultation pathway follows NICE guidelines for obesity management, beginning with BMI calculation and cardiovascular risk assessment, progressing through medication selection based on patient history and contraindications, and continuing with scheduled follow-up appointments to monitor weight loss progress and manage dose titration. Digital prescribing platforms such as RxSure provide pre-built weight management templates that guide prescribers through each clinical decision point, automatically check for drug interactions, generate private prescriptions with correct dosing schedules, and maintain the complete audit trail required for GPhC compliance.
Pharmacy group private prescribing for weight management has entered a new era. With 26% of adults in England classified as obese and a further 38% overweight according to NHS Digital’s Health Survey for England 2023, the demand for effective pharmacological weight loss interventions has never been higher. GLP-1 receptor agonists — particularly semaglutide and tirzepatide — have transformed the treatment landscape, offering clinically significant weight reduction that was previously achievable only through bariatric surgery.
For pharmacy groups operating across multiple sites, the question is no longer whether to offer GLP-1 weight management services, but how to deliver them safely, consistently, and at scale. The operational complexity of running these services — cold chain logistics, patient monitoring protocols, prescriber oversight, and regulatory compliance — demands purpose-built digital infrastructure that generic pharmacy management systems simply cannot provide.
GLP-1 Market Growth: Semaglutide, Tirzepatide, and What Comes Next
The clinical pathway for prescribing GLP-1 medications in a pharmacy setting requires careful patient selection, structured monitoring, and adherence to evidence-based protocols. Patients must meet specific BMI thresholds, typically 30 or above, or 27 with weight-related comorbidities such as type 2 diabetes, hypertension, or obstructive sleep apnoea, before GLP-1 therapy can be initiated. The prescriber must assess cardiovascular risk, thyroid history including family history of medullary thyroid carcinoma, and current medications for potential interactions. Semaglutide requires a dose titration schedule starting at 0.25 milligrams weekly and increasing over sixteen weeks to the maintenance dose, while tirzepatide follows its own titration protocol. Follow-up consultations should be scheduled at four-week intervals during titration to assess tolerability, monitor for gastrointestinal side effects, and adjust dosing as needed. A digital platform with guided consultation workflows ensures that prescribers follow these clinical steps consistently for every patient, reducing the risk of missed safety checks and providing documentation that satisfies regulatory inspection requirements.
The numbers tell a compelling story. NICE approved semaglutide (Wegovy) for weight management in 2023, and NHS England began rolling out specialist obesity services shortly after. However, NHS provision remains severely constrained — waiting lists for tier 3 weight management services exceed 12 months in most regions. This gap between clinical need and NHS capacity has created enormous demand for private prescribing.
Tirzepatide (Mounjaro), a dual GIP/GLP-1 receptor agonist, received MHRA authorisation for weight management in late 2023, demonstrating weight loss of up to 22.5% of body weight in clinical trials — the SURMOUNT-1 trial data that caught global attention. With both molecules now available privately, pharmacy groups are positioning themselves as accessible, clinically governed providers of these treatments.
The UK weight management market is projected to exceed £1 billion annually by 2027, according to industry analysis from IQVIA. Pharmacy groups that invest in robust platform infrastructure now will capture significant market share, while those relying on manual processes risk being unable to scale safely.
Operational Challenges of Multi-Site GLP-1 Services
Running a GLP-1 weight management service from a single pharmacy is manageable with spreadsheets and manual processes. Running it across ten, twenty, or fifty sites is an entirely different proposition. The challenges multiply exponentially:
- Cold chain management — semaglutide and tirzepatide require refrigerated storage at 2-8°C. Each site needs temperature monitoring, stock rotation tracking, and real-time visibility of expiry dates across the group.
- Dose titration protocols — GLP-1 agonists follow strict titration schedules (semaglutide: 0.25mg → 0.5mg → 1mg → 1.7mg → 2.4mg over 16+ weeks). Patients moving between sites need seamless continuity.
- Patient monitoring — regular weight checks, BMI tracking, adverse effect screening, and assessment of contra-indications at each dose increase. Miss a check and you risk patient harm.
- Prescriber capacity planning — independent prescriber availability must match patient demand across all sites, with appropriate skill mix for initial assessments versus follow-up reviews.
- Stock allocation — global supply constraints have affected semaglutide availability. Groups need intelligent stock distribution based on patient commitments, not first-come-first-served.
Platform Requirements for Pharmacy Group Weight Management
What does a digital platform need to deliver to support GLP-1 services at scale? Based on the operational realities above, the requirements fall into several categories that generic pharmacy systems rarely address.
Centralised Patient Records with Multi-Site Access
A patient who starts their weight management journey at your Manchester branch and collects their next injection at your Leeds site must have a single, unified clinical record. The prescriber in Leeds needs immediate visibility of the Manchester consultation notes, the current titration stage, the last recorded weight, and any adverse effects reported. Platforms like RxSure can provide this unified view, eliminating the dangerous information gaps that occur when sites operate in isolation.

Automated Titration Scheduling and Alerts
Manual diary management for dose titrations becomes unworkable beyond a handful of patients. A platform should automatically schedule the next dose increase, flag patients due for review, and alert prescribers to any missed appointments or monitoring requirements. When a patient is three days overdue for their week-four weight check, the system should escalate — not wait for someone to notice.
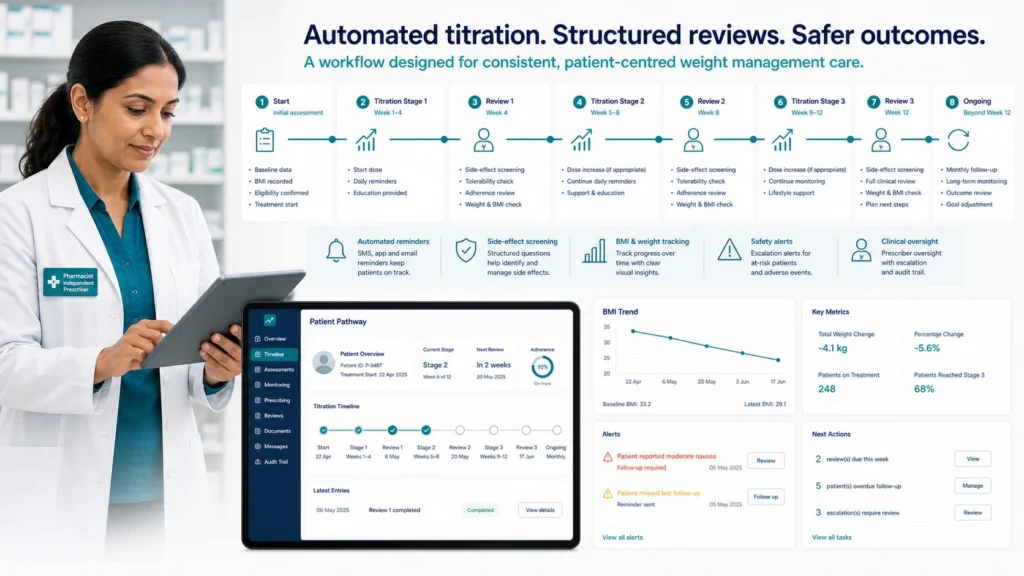
Clinical Governance Dashboards
Clinical leads and superintendent pharmacists need real-time oversight without manually reviewing individual patient records. Key metrics include: percentage of patients achieving clinically significant weight loss (5%+ at 12 weeks), adverse effect incidence rates, dropout rates by site, prescriber activity volumes, and compliance with monitoring protocols. If one site shows unusually high dropout or low efficacy, that signals an operational or clinical issue requiring investigation.
Compliance and Audit Trail
The GPhC expects pharmacy owners to demonstrate robust clinical governance. Every prescribing decision, every patient interaction, every dose change must be recorded with timestamps, prescriber identification, and clinical rationale. When the inspectors visit — and they will, given the high-profile nature of GLP-1 prescribing — your audit trail must be comprehensive and instantly retrievable.
Cold Chain and Supply Management at Scale
GLP-1 medications represent a significant financial investment for pharmacy groups. A single pen of semaglutide 2.4mg costs upwards of £170 wholesale. A group holding stock across twenty sites could easily have £200,000 of temperature-sensitive inventory at any given time. Robust stock management is not optional — it is a financial imperative.

Platform features that support cold chain management include:
- Batch tracking — linking specific batches to specific patients for recall capability
- Expiry date monitoring — flagging stock approaching expiry for prioritised dispensing or inter-site transfer
- Temperature excursion logging — integrating with digital temperature monitoring to flag stock that may have been compromised
- Demand forecasting — predicting stock requirements based on active patient numbers and titration schedules per site
Without these capabilities, pharmacy groups face wastage from expired stock, patient delays from stock-outs, and potential patient safety issues from compromised cold chain products.
Prescriber Oversight and Clinical Safety
Weight management prescribing carries specific risks that demand robust oversight. NICE guidelines (CG189 and TA875) set clear criteria for who should receive GLP-1 treatment: BMI ≥30 kg/m² (or ≥27 with weight-related comorbidities), alongside lifestyle interventions. Prescribers must also screen for contraindications including personal or family history of medullary thyroid carcinoma, MEN2, pancreatitis, and severe gastrointestinal disease.
A platform supporting multi-site GLP-1 services should enforce these criteria through structured clinical pathways. Rather than relying on individual prescriber memory, the system should present mandatory screening questions, flag contraindications automatically, and prevent prescribing outside agreed protocols without clinical lead override. This is not about removing clinical judgement — it is about supporting consistent, safe decision-making across dozens of prescribers.
Learn more about how partnership models can support your clinical governance framework.
How Digital Platforms Enable Scalable Weight Management
The pharmacy groups successfully scaling GLP-1 services share common characteristics. They have invested in digital infrastructure that removes manual bottlenecks, standardises clinical processes, and provides real-time visibility across their entire operation. They are not working harder — they are working smarter.
Consider the patient journey through a digitally-enabled pharmacy group versus a manual operation:
- Booking — online self-service versus telephone tag with reception staff
- Pre-screening — automated eligibility questionnaire versus prescriber time spent on basic criteria checking
- Consultation — structured clinical pathway with decision support versus free-text notes varying by prescriber
- Follow-up — automated scheduling with patient reminders versus manual diary management
- Monitoring — dashboard alerts for overdue patients versus hoping someone remembers to check
Each of these improvements compounds. A group seeing 500 weight management patients per month across 15 sites saves hundreds of administrative hours while simultaneously improving clinical safety. That is the operational case for platform investment.
Frequently Asked Questions
What qualifications do prescribers need to offer GLP-1 weight management services?
Prescribers must be registered independent prescribers (pharmacist IPs, nurse IPs, or doctors) with appropriate competency in weight management. The RPS recommends specific training in obesity pharmacotherapy, and many pharmacy groups require completion of a weight management credentialing programme. The GPhC expects prescribers to work within their competence and maintain a portfolio of CPD evidence in this therapeutic area.
How do pharmacy groups manage GLP-1 supply shortages?
Supply constraints have been a persistent challenge since 2023. Effective strategies include maintaining relationships with multiple wholesalers, using platform-based demand forecasting to order proactively, implementing patient waiting lists with transparent communication, and having agreed protocols for dose-holding during shortages. Some groups also offer alternative GLP-1 options (liraglutide) as bridging treatment when first-choice agents are unavailable.
What monitoring is required for patients on GLP-1 treatment?
At minimum: weight and BMI at each dose titration (typically every 4 weeks during escalation), assessment of gastrointestinal side effects, screening for signs of pancreatitis or gallbladder disease, and review of treatment efficacy at 12 weeks. NICE recommends discontinuation if less than 5% weight loss is achieved by 12 weeks on the maintenance dose. Regular HbA1c monitoring is also advisable in patients with pre-diabetes or diabetes.
Can pharmacy groups offer GLP-1 services without a digital platform?
Technically yes, but practically it becomes unsafe beyond a small scale. Manual processes introduce unacceptable risk when managing hundreds of patients on titrating injectable medications across multiple sites. The CQC and GPhC increasingly expect digital systems that support clinical governance, audit capability, and patient safety. Groups without platform support will struggle to evidence safe practice at inspection.
Sources & References
- National Institute for Health and Care Excellence. Obesity: identification, assessment and management (NG246). NICE, 2024.
- British National Formulary. BNF Online — Semaglutide, Tirzepatide, Orlistat. NICE, 2024.
- General Pharmaceutical Council. Standards for Pharmacy Professionals. GPhC, 2024.
Taking the Next Step
If your pharmacy group is planning to launch or scale GLP-1 weight management services, the platform decision is foundational. Getting it right means safer patients, more efficient operations, and the ability to grow without proportional increases in overhead. Getting it wrong means clinical risk, operational chaos, and regulatory exposure.
Explore how RxSure’s platform can support multi-site weight management services through our partnership programme, or get in touch to discuss your specific requirements. View our full pricing structure to understand the investment involved.
About this article: This article was prepared by the RxSure editorial team and is informed by publicly available UK healthcare guidance. Source references include GPhC, NICE, and BNF where cited. Content is reviewed periodically to reflect current information. This article is for general informational purposes and should not be relied upon as professional, medical, or regulatory advice. Last updated: 23 May 2026.