TL;DR: Learn how councils can digitise stop smoking services through community pharmacy, cutting costs per quit and improving outcomes with digital prescribing platforms.
Commissioning digital prescribing NHS pathways for smoking cessation is one of the most impactful decisions a council public health team can make today. Smoking remains the single largest preventable cause of death in England, responsible for approximately 76,000 deaths annually and costing the NHS an estimated £2.5 billion per year in direct treatment costs. Yet despite decades of investment, council-commissioned stop smoking services are reaching fewer people than ever — and the delivery model is largely stuck in the pre-digital era.
Community pharmacy offers a solution. With over 11,500 pharmacies across England — more accessible than GP surgeries, open longer hours, and staffed by qualified healthcare professionals — the network represents an extraordinary infrastructure for delivering smoking cessation at scale. What is missing is the digital connective tissue that would allow councils to commission, monitor, and evaluate these services efficiently.
The Scale of the Problem: UK Smoking Statistics in 2026
Private prescribing services delivered through UK community pharmacies and clinics have expanded rapidly in recent years, driven by the growing number of pharmacist independent prescribers, increasing patient demand for accessible healthcare outside traditional GP pathways, and the development of digital platforms that simplify clinical governance and regulatory compliance. The General Pharmaceutical Council has supported this expansion by maintaining clear standards for prescribing practice while allowing practitioners to develop their clinical scope based on competence and training. For practitioners, the key to successful private prescribing is combining clinical expertise with efficient operational processes that ensure every consultation is properly documented, every prescription meets regulatory requirements, and every patient receives appropriate follow-up care. Digital prescribing platforms provide the infrastructure to achieve this by offering structured consultation workflows, automated drug interaction checking, electronic prescription generation, compliance toolss, and complete audit trails that satisfy inspection requirements from both the GPhC and the Care Quality Commission.
Before examining digital solutions, it is worth grounding the discussion in current data. According to the Office for National Statistics (ONS) Annual Population Survey published in late 2025:
- 12.7% of adults in England smoke (approximately 5.4 million people)
- Smoking prevalence varies dramatically by region: 8.9% in the South East versus 17.3% in the North East
- Smoking rates in routine and manual occupations remain stubbornly high at 23.4%
- Only 37% of smokers who want to quit accessed any form of cessation support in 2024
The NHS Long Term Plan set a target of reducing smoking prevalence to below 5% by 2030 — a target that current trajectories will not meet without significant service redesign. The Office for Health Improvement and Disparities (OHID) has been explicit: new delivery models are needed, and community pharmacy must play a central role.
How Council Stop Smoking Services Currently Operate
Choosing the right technology platform for private prescribing services is a critical business decision that affects clinical workflow efficiency, regulatory compliance capability, patient experience, and long-term operational costs. The UK market offers several approaches including per-consultation fee platforms that charge for each prescription generated, marketplace models that aggregate patients across multiple practitioners, custom-built systems that require significant upfront development investment, and flat-rate subscription platforms that provide unlimited access to all features for a fixed monthly fee. Key evaluation criteria should include the comprehensiveness of the clinical workflow covering booking, consultation, prescribing, and follow-up in a single system, the quality of compliance features including audit trails, controlled drug management, and inspection-preparation reporting, integration capabilities with video consultation tools and payment processors, and the total cost of ownership calculated against realistic consultation volumes. Flat-rate platforms typically offer the best value for practitioners conducting more than fifteen consultations per month, as per-consultation charges accumulate quickly and can significantly erode consultation revenue at higher volumes.
Most council-commissioned stop smoking services follow a model established in the early 2000s:
- Specialist stop smoking advisors employed by the council or an outsourced provider deliver one-to-one or group behavioural support
- Pharmacotherapy (NRT, varenicline, or cytisine) is prescribed by GPs or provided via community pharmacy under a Patient Group Direction (PGD) or locally commissioned service
- Carbon monoxide monitoring validates quit status at 4 and 12 weeks
- Data collection happens via paper forms, spreadsheets, or bespoke local databases with limited interoperability
This model has significant limitations. Service access depends on appointment availability during working hours. Data flows between pharmacies, GP surgeries, and the commissioning council are fragmented. Outcome reporting to OHID is manual and often delayed. And the cost per quit — the key metric for commissioners — remains stubbornly high at £500-£1,200 per successful 4-week quit in many areas.
Why Community Pharmacy is the Natural Delivery Point
Community pharmacies offer structural advantages that no other healthcare setting can match for smoking cessation delivery:
- Accessibility: 89% of the English population lives within a 20-minute walk of a pharmacy (PSNC data, 2024)
- No appointment needed: Walk-in access removes a primary barrier to service uptake
- Extended hours: Many pharmacies open evenings and weekends, reaching working-age smokers
- Trusted professionals: Pharmacists are consistently rated among the most trusted healthcare professionals in public surveys
- Existing relationship with smokers: Pharmacies already supply NRT and interact daily with people who smoke
- Clinical capability: Pharmacist independent prescribers can prescribe all smoking cessation medications directly
The Pharmacy First programme, which expanded in January 2024, demonstrated that pharmacies can deliver clinical services at scale when properly supported with digital infrastructure and clear commissioning frameworks. Smoking cessation is a natural extension of this model.
The Digital Gap: Why Current Systems Fail Commissioners
Council public health teams face persistent frustrations with current stop smoking service delivery:
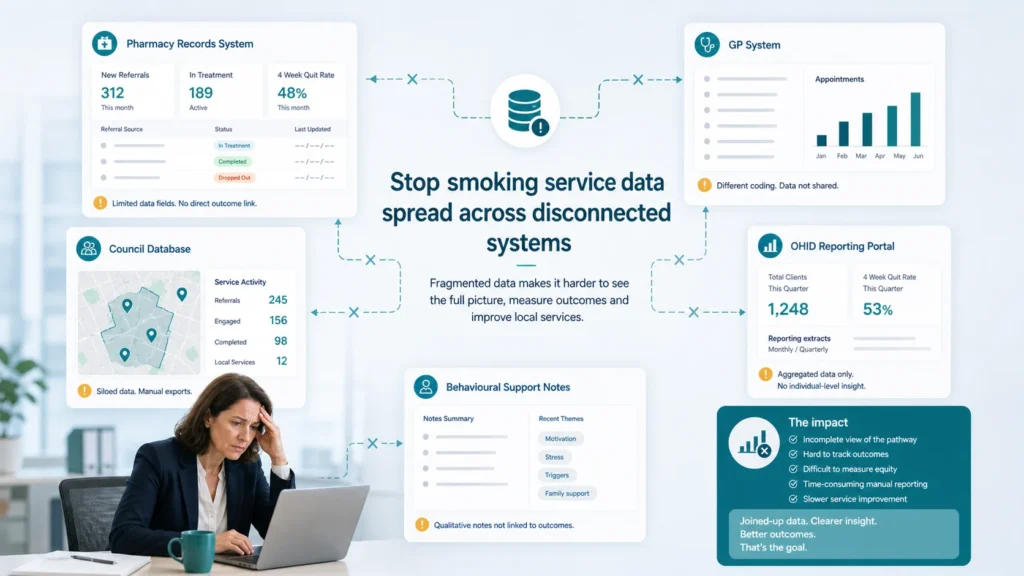
Data Fragmentation
Information about a single patient’s quit journey may exist across four or five separate systems: the pharmacy’s PMR (Patient Medication Record), the GP clinical system, the council’s commissioned service database, the OHID reporting portal, and potentially a separate system for the behavioural support provider. No single view of the patient journey exists, making it impossible to identify where drop-off occurs or which interventions are most effective.
Manual Reporting Burden
Pharmacies participating in commissioned smoking cessation services spend significant time on manual data entry and reporting. Research published by the University of Bath (2024) found that community pharmacies spend an average of 2.3 hours per week on administrative tasks related to commissioned service reporting — time that could be spent delivering patient care. This administrative burden actively deters pharmacies from participating in commissioned services.
Limited Real-Time Visibility
Commissioners typically receive outcome data quarterly, sometimes with an additional 6-8 week delay. This means a poorly performing service can operate for months before problems are identified. In contrast, a digital platform could provide real-time dashboards showing patient engagement, medication adherence, CO validation rates, and quit outcomes as they happen.
What Digital Transformation Looks Like for Smoking Cessation
A digitised council stop smoking service delivered through community pharmacy could operate as follows:
Patient Journey
- Self-referral: Patients access the service via a council-branded web portal or are referred digitally by their GP, midwife, or other healthcare professional
- Pre-screening: An online clinical questionnaire captures smoking history, medical history, and medication preferences
- Pharmacy allocation: The patient selects their preferred local pharmacy from a map of participating sites
- Clinical assessment: A pharmacist independent prescriber conducts a face-to-face or video assessment, with clinical data pre-populated from the referral
- Prescribing: The prescriber issues a private prescription for varenicline, cytisine, or NRT, recorded directly in the digital platform
- Behavioural support: Scheduled check-ins (digital or in-pharmacy) at weeks 1, 2, 4, 8, and 12
- CO validation: Results recorded digitally with automatic reporting to the commissioner
- Outcome reporting: Real-time data flows to the council’s public health team and OHID

Commissioner Dashboard
A digital platform provides commissioners with capabilities that manual systems simply cannot offer:
- Real-time quit rates by pharmacy, ward, and demographic group
- Cost-per-quit calculations updated automatically
- Patient drop-off analysis identifying where in the journey people disengage
- Prescribing pattern analysis showing medication effectiveness
- Health inequalities data mapped to Index of Multiple Deprivation (IMD) deciles
- Automatic OHID reporting compliance
The Commissioning Framework: How Councils Can Procure Digital Services
Local authority public health teams commission services under Section 7A of the NHS Act 2006 (as amended). Smoking cessation sits within the public health grant, which totalled £3.4 billion across England in 2025/26. However, the public health grant has been subject to real-terms cuts of approximately 26% since 2015/16 (Health Foundation analysis), making efficiency gains through digital delivery essential rather than optional.
Procurement routes for digital smoking cessation services include:
- Direct award: For contracts below the council’s procurement threshold (typically £50,000-£100,000), a direct award to a suitable provider may be possible
- Framework agreements: Several NHS and local government frameworks include digital health services (including G-Cloud and the Health Systems Support Framework)
- Competitive tender: For larger contracts, a full procurement exercise with clinical and technical evaluation criteria
- Innovation partnerships: Some councils are using innovation partnership procedures to co-develop digital solutions with technology providers
Evidence Base: What Works in Digital Smoking Cessation
The evidence supporting digital approaches to smoking cessation is growing rapidly:
- NICE guideline NG209 (updated 2023) explicitly supports digital delivery of behavioural interventions for smoking cessation
- A Cochrane review (Whittaker et al., 2019, updated 2023) found that mobile phone-based interventions increased quit rates by 50-60% compared to control
- The NHS Smokefree app has demonstrated that digital engagement tools can complement clinical services effectively
- PHE (now OHID) local tobacco control profiles show that areas with digital referral pathways achieve 23% higher service uptake than those relying solely on traditional referral routes
NICE Technology Appraisal 123 (updated) and the NICE pathway for smoking cessation both emphasise the importance of accessible, evidence-based services delivered in community settings. Digital platforms that enable pharmacy-based delivery align directly with this guidance.
How Platforms Like RxSure Could Support This Transformation
Prescribing platforms designed for independent prescriber-led services can provide the digital infrastructure that council smoking cessation services need. A platform like RxSure could offer:
- Clinical workflow management: Structured assessment pathways for smoking cessation that guide prescribers through NICE-compliant consultations
- Prescribing capability: Pharmacist independent prescribers can assess and prescribe directly within the platform, eliminating GP referral delays
- Outcome tracking: Automated 4-week and 12-week quit outcome recording with CO validation integration
- Commissioner reporting: Real-time dashboards and automated OHID data submissions
- Patient engagement: Digital check-in reminders, behavioural support content, and medication adherence tracking
- Multi-pharmacy coordination: A single platform connecting all commissioned pharmacies within a council area
For more information about how the platform’s clinical features support commissioned service delivery, or to explore pricing models suitable for council commissioning budgets, visit our dedicated pages.
Implementation Considerations for Commissioners
Council public health teams considering digital transformation of smoking cessation services should plan for:
- Pharmacy recruitment: Not all pharmacies will have independent prescribers. A mixed model (IP pharmacies for prescribing, all pharmacies for NRT supply and behavioural support) may be needed initially
- Digital inclusion: Not all smokers are digitally confident. Services must maintain non-digital access routes alongside the digital platform
- Data sharing agreements: Information governance arrangements between the council, pharmacies, and the technology platform require formal Data Sharing Agreements
- Training: Pharmacy teams need orientation to the digital platform, typically 2-4 hours of initial training
- Change management: Moving from paper-based to digital reporting requires active change management, particularly with established pharmacy teams

Financial Modelling: The Case for Digital Investment
A typical council commissioning area (population 250,000, approximately 30,000 adult smokers) might model the following comparison:
Traditional service model (annual costs):
- Specialist advisors (3 FTE): £120,000
- Premises and overheads: £35,000
- Pharmacotherapy costs: £80,000
- Administration and reporting: £25,000
- Total: £260,000 for approximately 400 4-week quits (cost per quit: £650)
Digital pharmacy model (annual costs):
- Digital platform licence: £36,000-£60,000
- Pharmacy service fees (per-patient): £90,000
- Pharmacotherapy costs: £95,000
- Programme management: £30,000
- Total: £251,000-£275,000 for approximately 550-650 4-week quits (cost per quit: £420-£500)
The digital model delivers more quits at a lower cost per quit, primarily because pharmacy accessibility drives higher service uptake and the reduced administrative burden allows more time for patient-facing care.
Sources & References
- General Pharmaceutical Council. Standards for Pharmacy Professionals. GPhC, 2024.
- National Institute for Health and Care Excellence. NICE Guidelines. NICE, 2024.
- British National Formulary. BNF Online. NICE, 2024.
- Information Commissioner’s Office. Guide to UK GDPR. ICO, 2024.
Frequently Asked Questions
Can community pharmacies legally prescribe smoking cessation medications under a council-commissioned service?
Yes, through two primary routes. First, pharmacist independent prescribers can prescribe any medication within their competence, including varenicline and cytisine. Second, pharmacies can supply NRT under Patient Group Directions commissioned by the local authority. The independent prescriber route offers greater clinical flexibility and eliminates the need for GP involvement, which is why digital platforms focused on IP-led services are particularly relevant for this commissioning model.
What data does OHID require from commissioned stop smoking services?
OHID collects data through the Stop Smoking Services (SSS) monitoring return, submitted quarterly. Required fields include patient demographics, quit date, pharmacotherapy used, 4-week and 12-week outcomes, CO validation status, and referral source. A digital platform can automate this data collection entirely, eliminating the manual quarterly reporting burden and improving data quality through structured capture at the point of care.
How do we ensure the service reaches smokers in the most deprived communities?
Community pharmacies are disproportionately located in areas of high deprivation — research by Todd et al. (2014, updated 2022) demonstrates that pharmacy density is highest in IMD deciles 1-3. This means a pharmacy-based digital service inherently reaches populations with the highest smoking prevalence. Commissioners can further target provision by offering enhanced incentives to pharmacies in priority wards, using the digital platform’s geo-mapping capabilities to identify service gaps.
What about the national Swap to Stop programme — does digital pharmacy delivery complement or compete with it?
The government’s Swap to Stop programme (launched 2023) distributes one million free vaping kits to smokers alongside behavioural support. A digital pharmacy-based cessation service complements Swap to Stop by providing the clinical assessment, pharmacotherapy prescribing, and structured follow-up that the vape distribution programme does not include. Many smokers benefit from pharmacotherapy alongside or instead of vaping, and a commissioned pharmacy service ensures clinical oversight of the quit attempt regardless of the product used.
Interested in exploring digital smoking cessation delivery for your council area? Platforms like RxSure can support local authority commissioners in designing and implementing pharmacy-based digital cessation services. Visit our partners page to understand commissioning partnership models, or contact us to discuss how digital prescribing infrastructure could support your local tobacco control objectives.
About this article: This article was prepared by the RxSure editorial team and is informed by publicly available UK healthcare guidance. Source references include GPhC, NICE, and BNF where cited. Content is reviewed periodically to reflect current information. This article is for general informational purposes and should not be relied upon as professional, medical, or regulatory advice. Last updated: 23 May 2026.