TL;DR: How pharmacy groups run separate prescribing practices across multiple sites on one platform. Role-based access, audit trails, and governance at scale.
The UK Pharmacy Group Landscape: Consolidation and Complexity
Multi-site pharmacy management presents unique operational challenges because private prescribing services must maintain consistent clinical standards, regulatory compliance, and patient experience across every location while allowing individual branches sufficient flexibility to respond to local demand. The key challenge is ensuring that standard operating procedures, clinical governance frameworks, and staff competency requirements are uniformly applied across all sites without creating excessive bureaucratic overhead that slows down service delivery. Centralised digital platforms address this by providing a single system of record that enforces standardised consultation workflows across all locations, aggregates compliance data into group-level dashboards, and enables regional managers to monitor performance metrics including consultation volumes, revenue, patient satisfaction scores, and audit completion rates across the entire group. Per-site branding capabilities allow each pharmacy to maintain its local identity on patient-facing materials including booking pages and prescription documents, while the underlying clinical and compliance infrastructure remains consistent. Staff management features track qualifications, training records, and credential expiry dates across all practitioners in the group.
Multi-site pharmacy software UK operators need has evolved dramatically over the past decade. The UK pharmacy sector is undergoing significant consolidation. While Boots (with over 1,800 branches) and Well Pharmacy (approximately 730 branches) dominate by volume, the most dynamic growth is occurring in independent pharmacy groups — clusters of 5 to 50 pharmacies operating under common ownership or partnership structures. The Company Chemists’ Association reports that group-owned pharmacies now account for over 60% of community pharmacies in England.
These groups face a unique operational challenge. Each pharmacy branch may offer different services, employ different prescribers with different competencies, serve different patient demographics, and operate under subtly different local commissioning arrangements. Yet the group needs centralised oversight for clinical governance, financial management, regulatory compliance, and strategic planning.
When private prescribing services are added to this mix — weight management, travel health, sexual health, dermatology — the complexity multiplies further. How do you maintain clinical standards across twenty prescribers in fifteen locations, each seeing different patient populations, while keeping everything auditable and compliant? The answer, increasingly, is a platform approach.
Why Generic Pharmacy Systems Fall Short
Scaling private prescribing services across multiple pharmacy or clinic locations requires a phased approach that proves the service model at a pilot site before rolling out to additional locations. The pilot phase should establish the clinical governance framework, test consultation workflows, validate pricing against local market demand, and identify any operational issues before the model is replicated. Key success metrics to evaluate before scaling include average consultations per week, patient satisfaction scores, prescribing error rates, compliance audit results, and financial performance including revenue per consultation and overall service profitability. Once the model is validated, expansion to additional sites should follow a structured rollout plan covering staff recruitment and training, premises preparation, equipment procurement, platform configuration, and local marketing activities. Centralised management platforms such as RxSure enable rapid rollout because new sites can be configured within the existing platform infrastructure, inheriting pre-built consultation templates, compliance frameworks, and reporting structures from the pilot site. This reduces setup time for each new location from weeks to hours and ensures consistency from day one.
Traditional pharmacy management systems — PharmOutcomes, Positive Solutions, Cegedim — were designed for dispensing workflows and NHS service delivery. They excel at processing prescriptions, managing stock, and handling MDS trays. But they were never architected for multi-site private prescribing with independent clinical governance per branch.
The limitations become apparent quickly:
- No multi-tenancy — most systems treat each branch as a completely separate installation, with no cross-site visibility or shared patient records
- Limited role-based access — pharmacy systems typically have ‘pharmacist’ and ‘counter staff’ roles, not the nuanced permissions needed for prescribing governance (clinical lead, prescriber, administrator, superintendent, auditor)
- No private prescribing workflow — built for NHS dispensing, they lack private prescription generation, clinical assessment templates, patient consent management, and follow-up scheduling
- Inadequate reporting — NHS service reporting is well-supported, but private prescribing KPIs (revenue per prescriber, consultation conversion rates, patient retention) are absent
- No patient portal — patients cannot book, complete pre-screening, or access their records through these systems
For pharmacy groups serious about private prescribing revenue, a purpose-built prescribing platform is not a luxury — it is the minimum infrastructure required to operate safely and efficiently at scale.
Role-Based Access: Getting Permissions Right
In a multi-clinic prescribing environment, who can see what — and who can do what — is not merely an administrative convenience. It is a clinical governance requirement and a regulatory expectation. The GPhC’s standards for registered pharmacies explicitly require that access to patient information is limited to those who need it for legitimate purposes.
A robust platform needs at minimum these role tiers:
- Superintendent Pharmacist — full visibility across all sites, ability to review any patient record, prescriber activity, and clinical decision. Cannot be restricted by branch.
- Clinical Lead (per site or regional) — oversight of prescribers within their scope, ability to audit consultations, approve complex cases, and manage formulary access within their region
- Independent Prescriber — access to their own patients across sites (if the patient moves between branches), ability to prescribe within their declared competence areas only
- Clinic Administrator — appointment management, patient communications, basic record access for scheduling purposes, no access to clinical notes or prescribing decisions
- Group Operations Manager — financial reporting, service utilisation metrics, capacity planning data. No access to individual patient clinical records.
- Auditor (external) — read-only access to anonymised or specific audit trails, time-limited, with full logging of their access

Platforms like RxSure can implement this granular role architecture, ensuring that each user sees precisely what they need — no more, no less.
Audit Trails: The Non-Negotiable Foundation
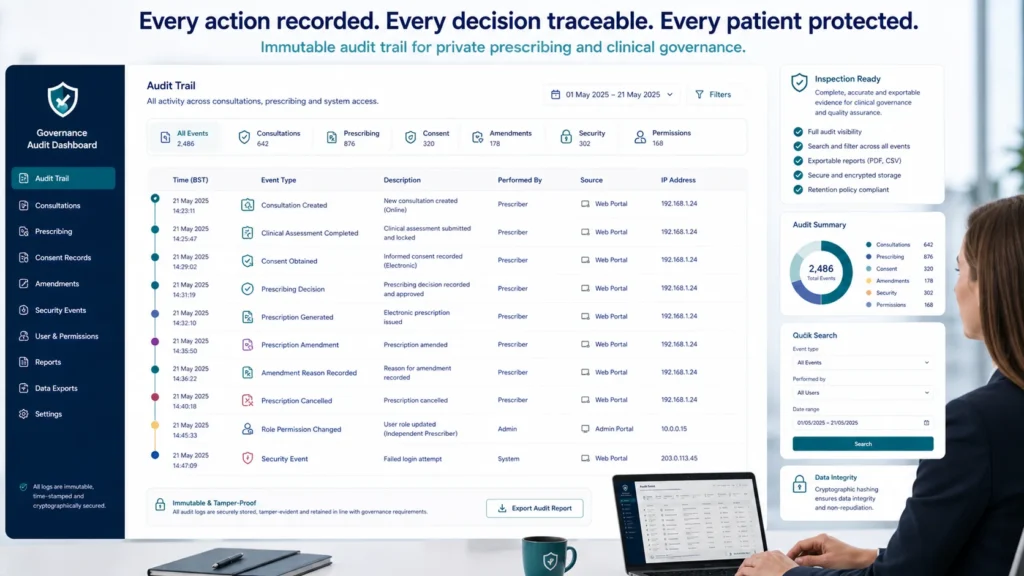
When the GPhC inspector sits down with your superintendent pharmacist and asks to see evidence of clinical governance, the audit trail is what separates a well-run group from one facing enforcement action. Every significant action within a multi-clinic prescribing platform must be logged immutably:
- Patient record creation and modification (who, when, what changed)
- Consultation start and end times with prescriber identification
- Clinical assessment data captured during consultation
- Prescribing decisions — including the clinical rationale documented by the prescriber
- Prescription generation and delivery method
- Prescription amendments or cancellations with reasons
- Patient consent records and withdrawal of consent
- Role and permission changes for any user
- Failed access attempts and security events
The CQC’s inspection framework for independent healthcare providers (which covers private prescribing services) specifically assesses whether providers can demonstrate effective governance through complete, accessible records. A comprehensive audit trail is not paranoia — it is professional survival.
Formulary Management Across Multiple Sites
Not every branch in a pharmacy group should prescribe everything. A branch with a prescriber competent in dermatology might offer acne and eczema services, while another with a travel health specialist focuses on malaria prophylaxis and travel vaccinations. The platform must support differentiated formularies without creating operational chaos.

Effective multi-site formulary management includes:
- Group-level master formulary — the complete list of medications the group is authorised to prescribe, maintained by the clinical governance committee
- Site-level formulary subsets — each branch can only access medications relevant to their active services, preventing scope creep
- Prescriber-level restrictions — individual prescribers are further limited to medications within their declared competence. A prescriber credentialed in weight management cannot suddenly prescribe dermatology treatments.
- Formulary change management — additions and removals go through an approval workflow (clinical lead recommendation → superintendent approval → system update), with full audit trail
- Pricing consistency — ensuring patients are charged consistently across sites for the same medication, with platform-enforced pricing rules
This layered approach ensures clinical safety while allowing operational flexibility. New services can be added to individual sites without affecting the wider group, and prescriber competence expansion is managed through a controlled process rather than ad hoc system access changes.
Centralised vs. Decentralised Clinical Governance
Pharmacy groups running multi-site prescribing face a fundamental governance design choice. Do you centralise all clinical oversight at group level, or devolve it to individual sites? In practice, the answer is usually a hybrid — but getting the balance right is critical.
Centralised Governance Benefits
- Consistent clinical standards across all sites — patients receive the same quality regardless of branch
- Efficient use of clinical lead time — one strong clinical lead can oversee multiple sites via platform dashboards
- Simplified regulatory interaction — one governance framework to present to GPhC and CQC inspectors
- Standardised training and CPD requirements for all prescribers
Decentralised Governance Benefits
- Faster local decision-making — site-level clinical leads can respond to local circumstances without group-level bottlenecks
- Service differentiation — branches can specialise in different therapeutic areas based on local demand and prescriber expertise
- Resilience — a governance issue at one site does not automatically cascade to affect the entire group’s operations
- Prescriber autonomy — experienced prescribers feel trusted rather than micromanaged
The optimal model for most pharmacy groups is centralised standards with decentralised execution. The group sets the clinical protocols, formulary boundaries, and training requirements. Individual sites and prescribers operate within those boundaries with appropriate autonomy. The platform enforces the boundaries automatically — prescribers physically cannot prescribe outside their credentialed scope — while dashboards give group-level visibility without requiring constant manual oversight.
Platform Features That Enable Multi-Clinic Efficiency
Beyond the governance fundamentals, what practical features should pharmacy group CEOs demand from a multi-clinic prescribing platform?
- Single patient record, multi-site access — a patient registered at one branch is visible (with appropriate permissions) at any branch in the group
- Cross-site appointment booking — patients can book at any branch through one portal, seeing real-time prescriber availability
- Group reporting dashboard — revenue, consultation volumes, prescriber utilisation, patient satisfaction, and clinical outcomes visible at group, regional, and site level
- Automated compliance monitoring — the platform flags when prescriber registrations are approaching renewal, when CPD requirements are unmet, or when consultation volumes suggest capacity issues
- Inter-site referral — if a patient needs a service only available at another branch, the referral is handled within the platform with full clinical context transfer
- Centralised communications — patient messaging, appointment reminders, and follow-up communications managed at group level for brand consistency
- Financial reconciliation — per-site revenue tracking, prescriber payment calculations, and group-level financial reporting integrated into one view
Each of these features eliminates manual work that scales linearly with branch count. A ten-branch group doing these tasks manually might need two full-time administrators. A fifty-branch group doing them manually needs ten. With platform automation, the overhead barely increases regardless of group size.
Regulatory Compliance for Multi-Site Operations
The regulatory landscape for pharmacy groups running private prescribing services involves multiple overlapping bodies. Understanding who expects what — and how your platform evidences compliance — is essential for operational peace of mind.
- GPhC — regulates the pharmacy premises and pharmacist registrants. Expects standards for registered pharmacies to be met at every site, with the superintendent pharmacist demonstrating oversight of all branches.
- CQC — if your prescribing service constitutes a regulated activity (treatment of disease, disorder, or injury), CQC registration may be required. Multi-site services may need a single registration with multiple locations, or separate registrations depending on structure.
- ICO — data protection compliance under UK GDPR. A multi-site group processing health data needs a comprehensive data protection framework, legitimate processing conditions, and likely a Data Protection Officer.
- NHS England — if any sites also deliver NHS services, the platform must maintain clear separation between NHS and private patient records and financial flows.
A well-designed platform generates the evidence these regulators need as a byproduct of normal operations. Inspections become straightforward when you can produce compliance reports at the click of a button rather than spending weeks collating spreadsheets.
Frequently Asked Questions
Can different branches within our group offer completely different services?
Absolutely. A well-architected platform supports service differentiation at branch level while maintaining group-wide governance standards. Branch A might offer weight management and travel health, Branch B might specialise in dermatology and sexual health, and Branch C might focus on women’s health. Each branch has its own service menu, formulary subset, and prescriber team — but all operate within the group’s overarching clinical governance framework and are visible on the group dashboard.
How do we handle prescribers who work across multiple branches?
This is increasingly common as groups optimise prescriber utilisation. The platform should support a prescriber being associated with multiple sites, with their schedule showing availability at each location. Their clinical permissions and formulary access remain consistent regardless of which branch they are working from. Patient records they create are attributed to the site where the consultation occurred, but remain accessible if they see the same patient at a different branch subsequently.
What happens if a prescriber leaves the group?
Platform-managed offboarding is critical. When a prescriber departs, their account is deactivated (never deleted — audit trail integrity requires the account to remain for historical records). Their active patients are flagged for reassignment to another prescriber. Any pending prescriptions are reviewed and either completed by another prescriber or cancelled with patient notification. The entire offboarding process is logged for governance purposes. GPhC professional register checks can be automated to flag unexpected deregistrations.
How does multi-site prescribing work with CQC registration?
CQC registration for multi-site prescribing typically follows one of two models. First, a single registration with multiple locations — the group registers once as a provider and adds each branch as a regulated location. This is simpler administratively but means a compliance failure at one site can affect the entire registration. Second, separate registrations per site — each branch registers independently. This provides isolation but increases administrative overhead significantly. Most pharmacy groups with fewer than twenty sites choose the single registration model. Your platform should support either approach with site-level compliance evidence generation.
Sources & References
- General Pharmaceutical Council. Standards for Pharmacy Professionals. GPhC, 2024.
- National Institute for Health and Care Excellence. NICE Guidelines. NICE, 2024.
- British National Formulary. BNF Online. NICE, 2024.
- Information Commissioner’s Office. Guide to UK GDPR. ICO, 2024.
Building Your Multi-Clinic Prescribing Operation
Running separate prescribing practices on one platform is not just technically possible — it is the approach that the most successful pharmacy groups are adopting nationwide. The combination of centralised governance, decentralised service delivery, and comprehensive platform automation creates operations that are simultaneously safer, more efficient, and more scalable than traditional manual approaches.
Whether your group operates five branches or fifty, the platform decision shapes everything that follows — from prescriber recruitment to service expansion to regulatory inspection outcomes. Invest in the right infrastructure now, and growth becomes a strategic choice rather than an operational constraint.
Discover how RxSure’s multi-clinic capabilities could support your pharmacy group’s prescribing ambitions through our partnership programme, or speak with our team about a tailored demonstration for your group’s specific requirements.
About this article: This article was prepared by the RxSure editorial team and is informed by publicly available UK healthcare guidance. Source references include GPhC, NICE, and BNF where cited. Content is reviewed periodically to reflect current information. This article is for general informational purposes and should not be relied upon as professional, medical, or regulatory advice. Last updated: 23 May 2026.