TL;DR: Transform your pharmacy appointment scheduling from chaos to clarity. Learn best practices for booking systems that reduce no-shows and improve patient flow.
Paper diary says 2pm. Computer calendar says 3pm. Email confirmation says tomorrow. The patient is standing at the counter expecting their appointment now.
This scenario or variations of it plays out in pharmacies daily. Multiple scheduling systems that do not communicate. Bookings made through different channels landing in different places. Staff unsure which schedule is authoritative.
The result: double bookings, missed appointments, frustrated patients, and stressed staff. All from something that should be straightforward: knowing when patients are coming.
The True Cost of Scheduling Problems
Patient Experience Impact
Scheduling failures directly damage patient relationships:
Double bookings: Patients wait while staff sort confusion, or get turned away despite valid appointments. Trust erodes.
Lost bookings: Patients say they booked but you have no record of it. Patients feel unvalued and may not return.
Inconvenient scheduling: Limited booking options mean patients cannot access services when needed. They go elsewhere.
No-show frustration: Patients who forget appointments waste slots other patients could use.
Operational Impact
Beyond patient experience, scheduling problems create operational chaos. Staff stress from dealing with booking problems while managing everything else increases pressure. Inefficient resource use means empty slots from no-shows sit next to rushed periods from overbooking. Revenue loss occurs because missed appointments mean missed service fees and empty consultation slots generate no income. Planning becomes impossible without reliable schedules since staffing and resource planning becomes guesswork.
Why Traditional Scheduling Fails
The Multiple System Problem
Many pharmacies accumulate scheduling approaches over time: paper diary for walk-ins, spreadsheet for vaccinations, email for private consultations, phone list for call-backs, and NHS system for commissioned services.
Each system works independently. None talks to the others. The result is fragmented scheduling with no single view of capacity.
The Channel Multiplication Problem
Patients now expect to book through multiple channels: phone calls, walk-in requests, website bookings, NHS app referrals, email requests, and social media messages.
Without integration, each channel creates its own scheduling stream, increasing double-booking risk.
Building an Effective Scheduling System
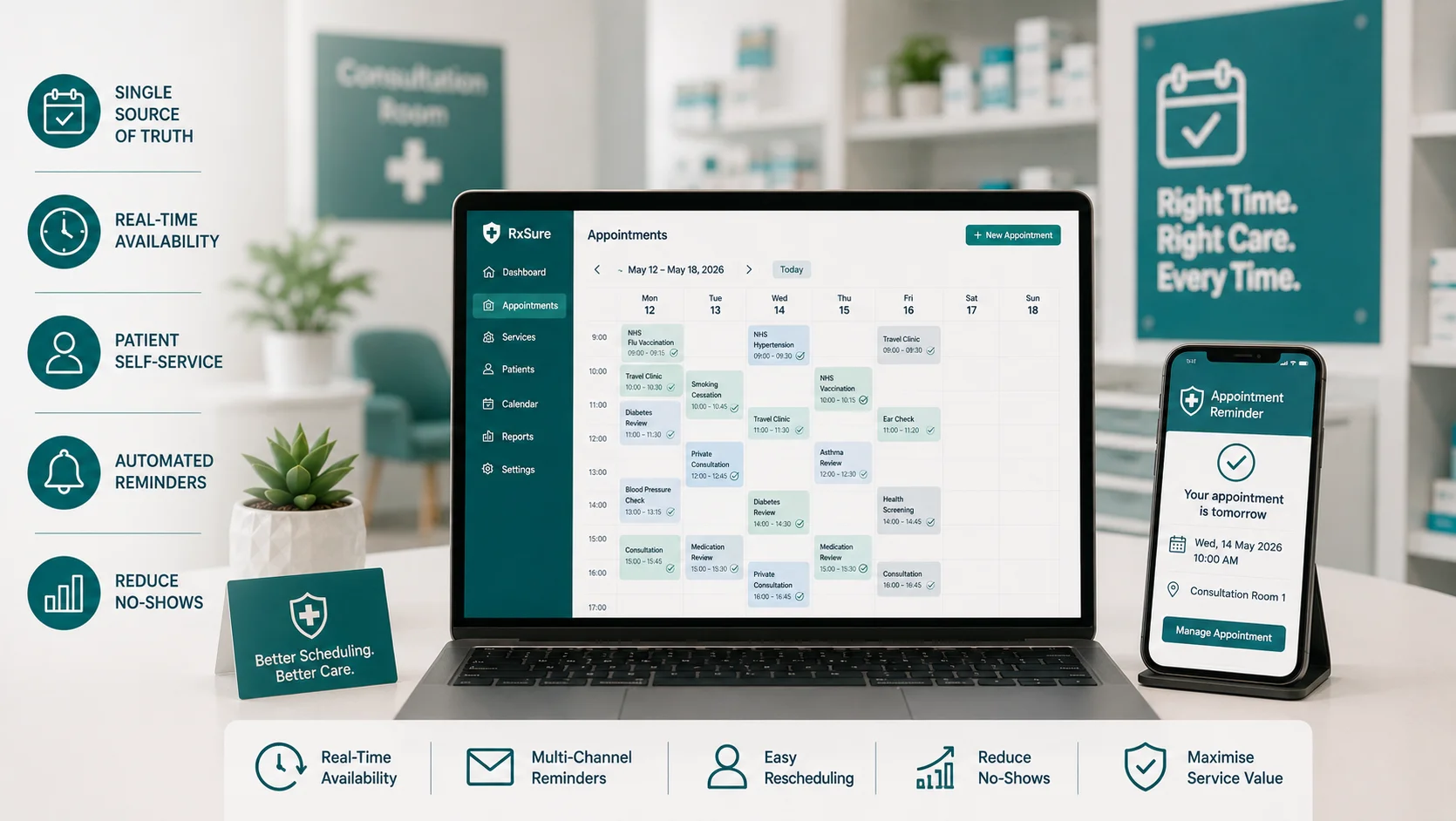
Principle 1: Single Source of Truth
All appointments, regardless of booking channel, must feed into one master schedule. This is non-negotiable. Without it, double bookings are inevitable.
Implementation requires choosing one primary scheduling system, ensuring all booking channels feed into it, training all staff to check this system only, and eliminating parallel scheduling tools.
Principle 2: Real-Time Availability
When a slot is booked, it must immediately become unavailable everywhere. Delay creates double-booking opportunity.
Implementation requires using systems with instant synchronisation, avoiding manual processes that create lag, and testing by booking simultaneously from different channels.
Principle 3: Patient Self-Service
Allow patients to book, change, and cancel appointments themselves where appropriate. This reduces admin burden and improves convenience.
Implementation includes online booking for suitable services, clear service descriptions and durations, automated confirmation and reminders, and easy cancellation and rebooking.
Principle 4: Automated Reminders
No-shows are dramatically reduced by timely reminders. Implement automated communication with booking confirmation sent immediately by email or SMS, 48-hour reminder allowing time to reschedule if needed, 24-hour reminder as final prompt, and optional day-of reminder for high-value services.
Principle 5: Buffer Time
Back-to-back appointments without buffer create knock-on delays when any appointment overruns. Build 5-10 minute buffers between appointments, longer buffers before complex services, and allow catch-up time periodically.
Service-Specific Scheduling Considerations
Vaccination Services
Allow batch booking for efficiency. Include 15-minute observation in slot length. Consider separate vaccination clinic times. Enable waitlist for cancellations.
Clinical Consultations
Use longer slots for complex consultations. Include patient preparation information in booking confirmation. Link private consultation room availability. Allocate appropriate pharmacist.
Commissioned Services
Ensure NHS system integration where required. Build in reporting capability. Link service-specific documentation. Automate outcome recording.
Reducing No-Shows
Understanding Why Patients Miss Appointments
Common reasons include simply forgetting, circumstances changed but felt awkward cancelling, did not value the appointment enough, transport or access problems, and health prevented attendance.
Strategies to Reduce No-Shows
Multiple reminders: SMS, email, and app notifications at strategic intervals.
Easy cancellation: Make it simple to cancel. A cancelled appointment can be rebooked. A no-show cannot.
Waitlists: Offer cancelled slots to waiting patients automatically.
Overbooking strategy: For services with predictable no-show rates, consider strategic overbooking.
Summary
Effective appointment scheduling transforms pharmacy operations. Patients access services conveniently, staff work efficiently, and revenue is protected. The key is one system, real-time updates, patient self-service, and automated reminders.
RxSure includes integrated appointment scheduling designed for pharmacy services. Online booking, automated reminders, real-time availability, and seamless integration with compliance tracking.
Start your free trial and transform your pharmacy scheduling.
About this article: This article was prepared by the RxSure editorial team and is informed by publicly available UK healthcare guidance. Source references include GPhC, NICE, and BNF where cited. Content is reviewed periodically to reflect current information. This article is for general informational purposes and should not be relied upon as professional, medical, or regulatory advice. Last updated: 4 July 2026.


